
Note: This article pertains mainly to offices in the Midwest, but you may find the information interesting if you live outside of the Midwest.
As you may have heard, Fulcrum/Chiropractic Care (a Minnesota-based, nonprofit physical medicine benefit management organization) will be ceasing contract operations effective August 31, 2026.
For those of you participating with Fulcrum, please watch your emails from Fulcrum and/or each payer group for further details and timelines. Whole Health Inc. will be taking over most of the below payer groups, and have advised some offices, via email, that they will be in contact.
We strongly recommend you ask Whole Health for a contract to review, along with a Fee Schedule.
Below is a sampling of what we know to date. Please refer to the FAQ included here Fulcrum Health Inc. for a full list of the payer groups impacted.
- Aetna/Allina
- Termination date with Fulcrum: 07/31/2026
- Contract through MultiPlan to stay in network (non-Minnesota), and SecureCare (Minnesota offices)
- Aspirus:
- Termination date with Fulcrum: 07/31/2026
- Aspirus is working on a transition plan; no further details at this time
- BPA
- Termination date with Fulcrum: 5/31/2026
- Claims for dates of service on or before 5/31/26 must be submitted to Fulcrum no later than end-of-day 7/17/26.
- No further details available at this time.
- Cigna
- Cigna will contract their chiropractic network through First Health.
- Quartz
- Termination date with Fulcrum: 6/30/2026
- Quartz will handle services in-house and will contract with provider groups only. They are focusing their outreach based on member utilization, geographic coverage & network needs. Provider groups that haven’t submitted claims within 12 months may not be contacted. If chosen, Quartz will send a group contract via Docu-sign and should have been received by 6/1/26.
- The Alliance
- Termination date with Fulcrum: 8/31/2026
- The Alliance is actively finalizing the contract and coordinating transition details with the new provider network partner. Once completed, their new provider network will reach out with next steps.
- Zelis
- Termination date with Fulcrum: 6/30/2026
- No further details available at this time; however, if you are credentialed and contracted directly with Zelis, you should not be impacted by this change.
- WPS
- Termination date with Fulcrum: 7/31/2026
- Fulcrum is sharing provider credentialing files with WPS. WPS may contact providers or providers may reach out to WPS at Provider Contracting.
- WPS informed me that the administration of their chiropractic network will transition to Chiropractic Management Services. To remain participating, providers will need to reach out to CMS Services LLC.
- WPS indicated their termination date with Fulcrum is 7/1/2026 (different than Fulcrum’s termination notice indicating termination on 7/31/26).
Additional Questions? We can help! And we will find an answer for you.
A big Thank you to Wisconsin’s Robyn Tozer for her work in helping to get initial updates – Thanks, Robyn!
Lisa


 As a follow-up to our previous compliance articles, I thought what I’d do this month is put together a FAQ list for my dear readers and call it Compliance 201. Keep reading to learn about upcoming new requirements in the compliance/cybersecurity world to keep you at least safe-guarded when you are hit with a cybersecurity incident. Special thanks and credit goes out to ChiroArmour and Dr. Scott Muensterman for his research and presenting at the Chiropractic Society of Wisconsin Fall Experience last month on some of the content in my FAQ.
As a follow-up to our previous compliance articles, I thought what I’d do this month is put together a FAQ list for my dear readers and call it Compliance 201. Keep reading to learn about upcoming new requirements in the compliance/cybersecurity world to keep you at least safe-guarded when you are hit with a cybersecurity incident. Special thanks and credit goes out to ChiroArmour and Dr. Scott Muensterman for his research and presenting at the Chiropractic Society of Wisconsin Fall Experience last month on some of the content in my FAQ.




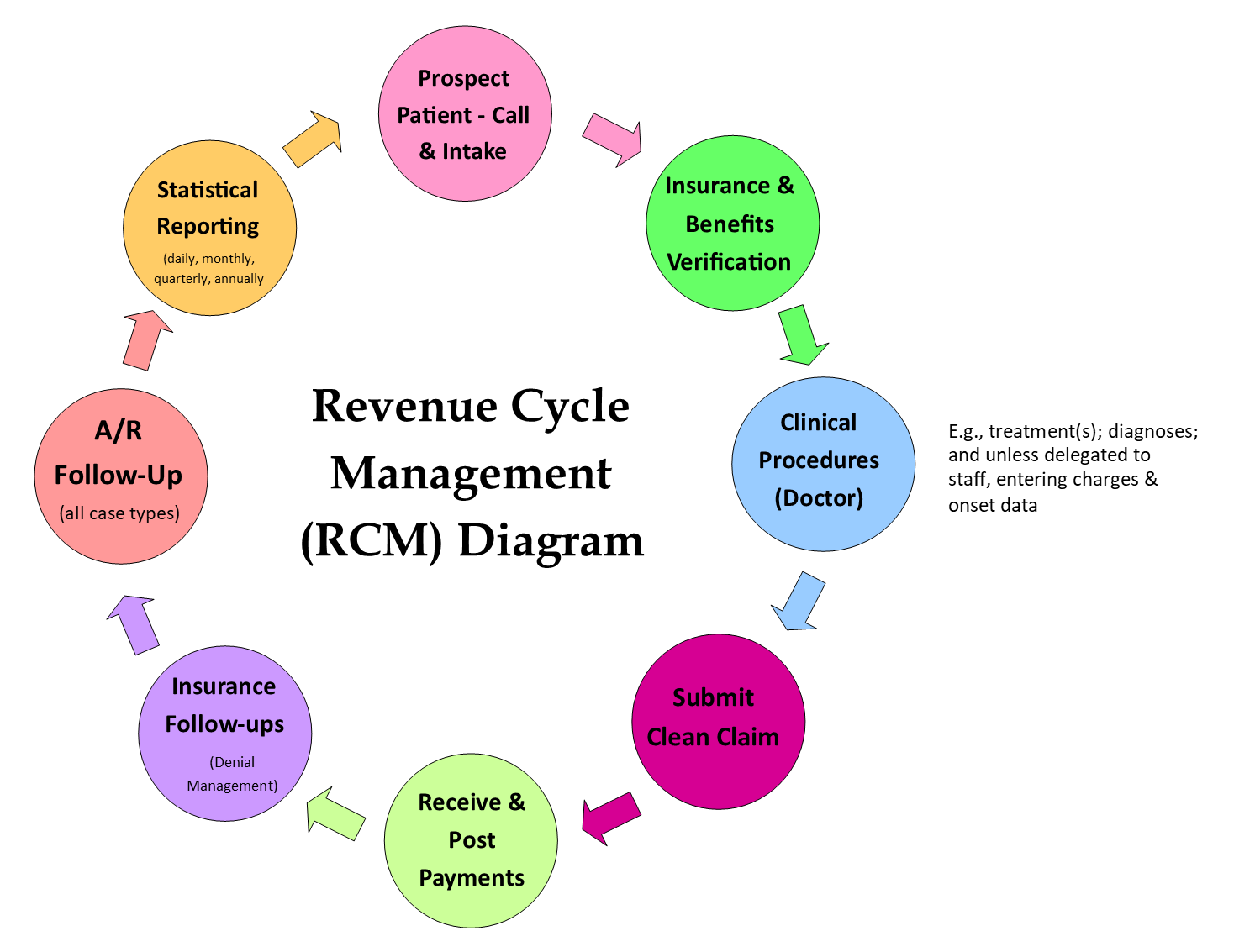 The important thing here is to be consistent, meaning every step and each element of the flow must align with the goals and mission of the clinic. For example, a pediatric/wellness practice will have different polices each step of the way for RCM than a sports medicine clinic would. If you are having issues, you need to examine which step in your RCM is bottlenecked, or which step is not in alignment.
The important thing here is to be consistent, meaning every step and each element of the flow must align with the goals and mission of the clinic. For example, a pediatric/wellness practice will have different polices each step of the way for RCM than a sports medicine clinic would. If you are having issues, you need to examine which step in your RCM is bottlenecked, or which step is not in alignment.
 Lisa recently had a phone conversation with United Healthcare for an update on the Change Healthcare Cyber Attack Update Regarding United Healthcare Payments & Remittances. UHC advises that they are close to a resolution on getting all of the clinic remittances available on the provider clearinghouses, and troubleshooting improper denials.
Lisa recently had a phone conversation with United Healthcare for an update on the Change Healthcare Cyber Attack Update Regarding United Healthcare Payments & Remittances. UHC advises that they are close to a resolution on getting all of the clinic remittances available on the provider clearinghouses, and troubleshooting improper denials.
 Bravery is one of the themes of our practice manager training program.
Bravery is one of the themes of our practice manager training program.
