Ever get the innate sense something is missing in bridging gaps you may be experiencing in your practice? As a result, you may tend to keep guessing and overthinking processes. Understandable from both a clinical perspective, and in today’s reimbursement landscape. Documenting and mapping out a business plan/practice roadmap can help calm the chatter.
According to Investopedia, “A business plan is a document that defines in detail a company’s objectives and how it plans to achieve its goals. A business plan lays out a written road map for the business from marketing, financial, and operational standpoints.”
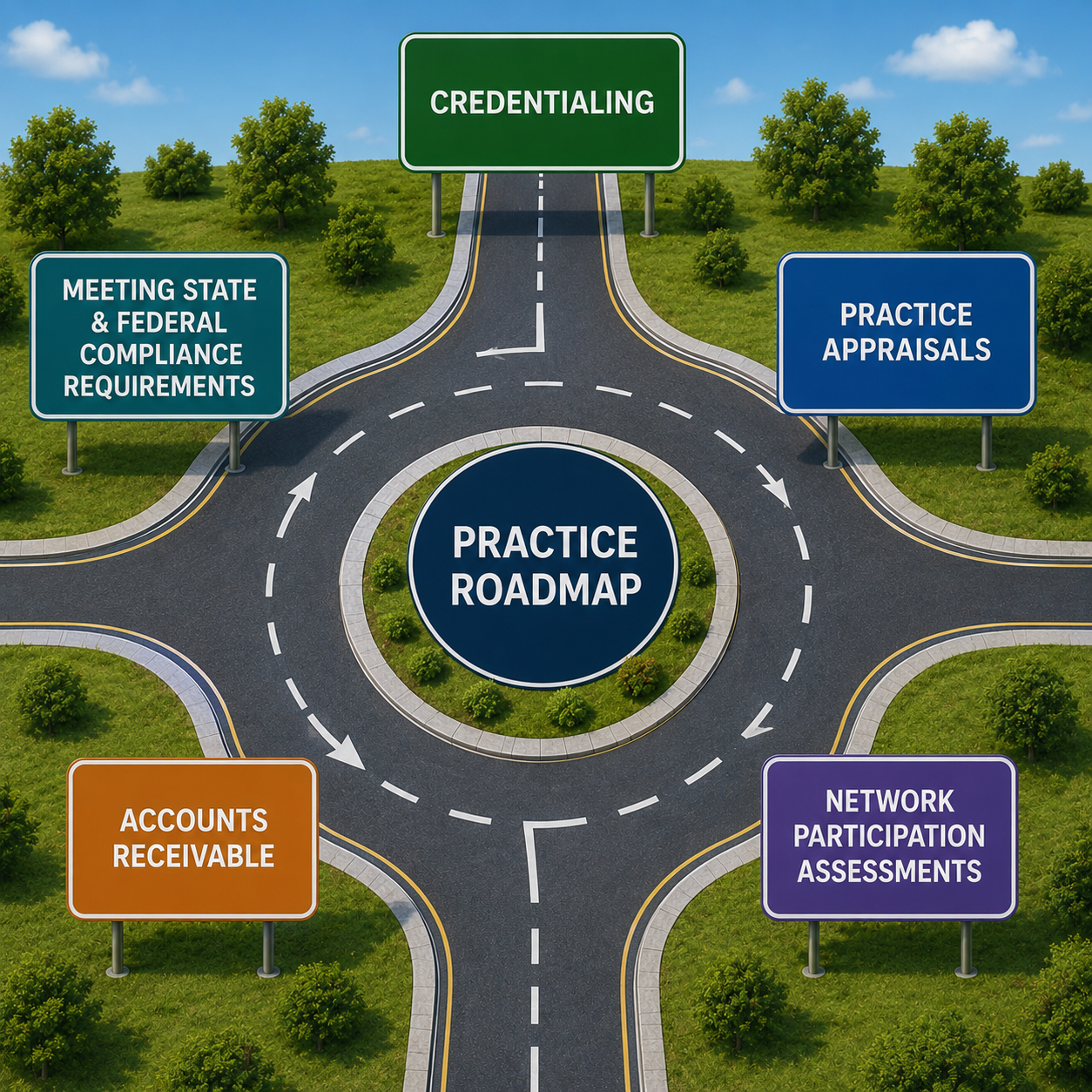
A business plan can help You navigate and evaluate the revenue cycle categories, which by the way are our specialties:
1.) Credentialing: The better HMO/PPO payer networks you participate in based on your geographic location and patient insurance type, the better the value of your practice.
2.) Practice Appraisals are a great foundation to your overall plan to see what your practice is worth at the time the appraisal is done.
3.) Network participation assessments: Have you recently ran reports on each payer group in your practice management software to see if you are getting reimbursed per contract? Where are any shortfalls you may want to voluntarily opt out of participating in? You’ll want to make sure you opt out of a network voluntarily, and intelligently – getting kicked out of a network involuntarily can bite you in the ass later on if you or your successor want to be in the network and continue filing insurance for patients. A common question on credentialing and re-credentialing requests is if you have ever been terminated involuntarily from a payer group or government program.
4.) Accounts Receivables: Where are your payer and patient receivables month to month? Is it increasing? Decreasing? According to Healthcare Financial Management Association (1), your ideal A/R percentages should fall here:
0–30 Days: ≥ 80% of your total A/R should fall into this category.
Over 90 Days: Less than 10% to 15% of your total outstanding A/R should be in this bucket.
Over 120 Days: Should ideally be kept under 15%. Accounts older than 180 days are often written off as bad debt.
If your financial policies are strong, you should have very little outstanding cash accounts over 90 days. Auto claims with attorneys and commercial secondaries should be about the only claims out in these categories.
5.)Meeting state and federal compliance requirements. Have you had a compliance assessment completed?
We can, have, and do help offices in each of these areas. Just Ask…
Lisa
Happy 250th Birthday, America!
 While at my desk on my physio ball, I was reading Chiropractic Economics annual Salary and Expense Surveys and took a deep dive into the Billing & Collections (B&C) category. I was jarred by a pattern over the past five years which makes me continue to fear that we are falling behind. The surveys in B&C category are a wake-up call that proves we can no longer ignore the impact of decreasing third-party reimbursements.
While at my desk on my physio ball, I was reading Chiropractic Economics annual Salary and Expense Surveys and took a deep dive into the Billing & Collections (B&C) category. I was jarred by a pattern over the past five years which makes me continue to fear that we are falling behind. The surveys in B&C category are a wake-up call that proves we can no longer ignore the impact of decreasing third-party reimbursements.

 As a follow-up to our previous compliance articles, I thought what I’d do this month is put together a FAQ list for my dear readers and call it Compliance 201. Keep reading to learn about upcoming new requirements in the compliance/cybersecurity world to keep you at least safe-guarded when you are hit with a cybersecurity incident. Special thanks and credit goes out to ChiroArmour and Dr. Scott Muensterman for his research and presenting at the Chiropractic Society of Wisconsin Fall Experience last month on some of the content in my FAQ.
As a follow-up to our previous compliance articles, I thought what I’d do this month is put together a FAQ list for my dear readers and call it Compliance 201. Keep reading to learn about upcoming new requirements in the compliance/cybersecurity world to keep you at least safe-guarded when you are hit with a cybersecurity incident. Special thanks and credit goes out to ChiroArmour and Dr. Scott Muensterman for his research and presenting at the Chiropractic Society of Wisconsin Fall Experience last month on some of the content in my FAQ.